COMPARATIVE ERGONOMIC RISK
ASSESSMENT OF MANUAL HANDLING TASKS
IN A SMALL-SCALE WATER BOTTLING
OPERATION USING RULA AND ERIN
Reina Verónica Román Salinas*
https://orcid.org/0000-0001-9287-4298
Facultad de Ingeniería Industrial,
Instituto Tecnológico Superior de Pánuco, México
Marco Antonio Díaz Martínez
https://orcid.org/0000-0003-1054-7088
Facultad de Ingeniería Industrial,
Tecnológico Nacional de México, México
Víctor Hugo Tobías Martínez
https://orcid.org/0009-0003-3555-1793
Área de Ingeniería y Ciencias,
Instituto de Ciencias y Estudios Superiores de Tamaulipas, México
Edgar Jearvavi Vázquez Moreno
https://orcid.org/0000-0002-3267-1445
Facultad de Ingeniería Industrial,
Tecnológico Nacional de México, México
Rubén Jérez Calderón
https://orcid.org/0009-0001-4778-2914
Facultad de Ingeniería Industrial,
Tecnológico Nacional de México, México
Received: March 17, 2026 / Accepted: April 23, 2026
Published: June 15, 2026
doi: https://doi.org/10.26439/ing.ind2026.n50.8671
ABSTRACT. Musculoskeletal disorders (MSDs) rank among the leading causes of occupational morbidity in manufacturing environments that demand high physical exertion. This study presents a comparative ergonomic risk assessment across five workstations at a small-scale water purification plant in Mexico, utilizing the RULA and ERIN assessment methods. We conducted a quantitative, non-experimental, cross-sectional analysis focusing on manual tasks involved in washing, rinsing, filling, sealing, and transporting 20 kg water containers. The ERIN method classified three workstations as high risk, with scores ranging from 28 to 35, while the RULA method identified one workstation as very high risk and two as high risk. The highest prevalence of musculoskeletal symptoms occurred in the wrist/hand (60 %) and lower back (55 %). The agreement between the two assessment methods facilitated the identification of critical factors related to arm posture, effort intensity, and work pace, thereby supporting the implementation of low-cost ergonomic interventions aimed at reducing the risk of MSDs.
KEYWORDS: ergonomic risk assessment / manual material handling / work-related musculoskeletal disorders / cumulative trauma disorders / RULA / ERIN
EVALUACIÓN COMPARATIVA DEL RIESGO ERGONÓMICO
EN TAREAS DE MANIPULACIÓN MANUAL EN UN PROCESO
DE EMBOTELLADO DE AGUA A PEQUEÑA ESCALA
UTILIZANDO RULA Y ERIN
RESUMEN. Los trastornos musculoesqueléticos (TME) constituyen una de las principales causas de morbilidad ocupacional en entornos de manufactura con altas demandas físicas. Este estudio realizó una evaluación comparativa del riesgo ergonómico en cinco estaciones de trabajo de una planta purificadora de agua en México mediante los métodos RULA y ERIN. Se desarrolló un estudio cuantitativo, no experimental y transversal, evaluando tareas de lavado, enjuague, llenado, sellado y transporte de garrafones de 20 kg. Los resultados de ERIN clasificaron tres estaciones en nivel de riesgo alto, con puntuaciones entre 28 y 35, mientras que RULA identificó una estación con riesgo muy alto y dos con riesgo alto. La mayor prevalencia de síntomas musculoesqueléticos se registró en muñeca/mano (60 %) y región lumbar (55 %). La concordancia entre ambos métodos permitió identificar factores críticos relacionados con postura del brazo, intensidad del esfuerzo y ritmo de trabajo, facilitando intervenciones ergonómicas de bajo costo.
PALABRAS CLAVE: evaluación del riesgo ergonómico / manipulación manual de materiales / trastornos musculoesqueléticos relacionados con el trabajo / trastornos por trauma acumulativo / RULA / ERIN
This research received no external funding.
* Corresponding author.
Author e-mails in order of appearance: [email protected], [email protected], [email protected], [email protected], [email protected]
This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0).
INTRODUCTION
Work-related musculoskeletal disorders (WMSDs) represent one of the most significant occupational health challenges globally. These conditions primarily arise from prolonged exposure to ergonomic risk factors, including awkward postures, repetitive movements, manual material handling, and sustained physical exertion during work tasks. Research has consistently shown that tasks involving manual material handling constitute a major source of biomechanical risk in production processes characterized by low levels of automation. This risk stems from the interplay of physical exertion, demanding postures, and repetitive movements, all of which increase the likelihood of developing musculoskeletal disorders among workers (Graziosi et al., 2024; Soares et al., 2026; Yang et al., 2023). Consequently, WMSDs serve as one of the leading causes of work-related disability and diminished productivity across various industrial sectors.
In this context, ergonomics serves a pivotal role in preventing occupational injuries and enhancing working conditions. This discipline specifically analyzes the interactions among workers, tools, and the work environment, aiming to design work systems that align with human capabilities while simultaneously promoting safety, well-being, and productivity. Systematic ergonomic assessments identify biomechanical risk factors and enable the development of intervention strategies to reduce the incidence of musculoskeletal disorders among workers (Demissie et al., 2024).
Among the tools used for ergonomic workstation evaluation, observational postural analysis methods have found extensive application in industrial environments to assess biomechanical exposure associated with various work tasks. Numerous studies have employed these methods to analyze postural load and musculoskeletal risks in manual material handling tasks, thereby demonstrating their effectiveness in identifying critical postures and suggesting ergonomic improvements in the workplace (Ansari & Sheikh, 2014; Conforti et al., 2019). A predominant method in this context is the Rapid Upper Limb Assessment (RULA), which facilitates the analysis of biomechanical load primarily affecting the upper limbs, neck, and trunk during task performance. RULA assigns risk scores based on the postures adopted by the worker, thus enabling the identification of situations that necessitate ergonomic intervention to prevent musculoskeletal injuries (McAtamney & Corlett, 1993; Muhacir et al., 2022).
The scientific literature indicates that observational methods rank among the most prevalent approaches for evaluating biomechanical workload in occupational settings, as they facilitate a systematic analysis of postural exposure, applied force, and movement repetition. However, no singular method adequately characterizes ergonomic exposure; thus, employing multiple assessment tools is advisable to achieve more comprehensive ergonomic evaluations (Takala et al., 2010).
Additionally, researchers developed the Ergonomic Risk Index (ERIN) as a comprehensive tool for assessing exposure to ergonomic risks associated with tasks that have a high physical demand. This tool considers variables related to posture, movement frequency, manual handling, and workplace conditions.
In conjunction with postural assessment tools, ergonomic studies frequently incorporate epidemiological instruments to analyze musculoskeletal symptoms in the working population. One of the most widely utilized instruments in this domain is the Nordic Musculoskeletal Questionnaire (NMQ), which assesses the prevalence of discomfort or pain in various body regions over specific time periods. The NMQ questionnaire has gained recognition as a well-validated tool in occupational health studies, owing to its capacity to correlate the incidence of musculoskeletal symptoms with working conditions and ergonomic risks (Crawford, 2007; Kuorinka et al., 1987).
Numerous studies in industrial settings reveal that a significant proportion of workers perform tasks under unfavorable ergonomic conditions, which heightens the risk of developing musculoskeletal disorders over time. Specifically, postural analyses utilizing observational methods indicate that many workers operate at moderate to high-risk levels. This finding underscores the need to implement corrective measures to improve workstation design and mitigate exposure to biomechanical risk factors (Grooten & Johansson, 2018; Yazdanirad et al., 2018).
Despite the expanding body of research in occupational ergonomics, there remains a need for studies that integrate observational and epidemiological tools to enhance the understanding of ergonomic risks, particularly in small-scale production processes that involve intensive manual material handling. Moreover, recent investigations have utilized sensor-based technologies, such as inertial measurement systems, to augment ergonomic assessments and improve the identification of musculoskeletal risk factors in occupational settings (Baklouti et al., 2024).
In this context, this study seeks to evaluate ergonomic risks by applying the RULA method and the ERIN index, and to analyze the prevalence of musculoskeletal symptoms with the Nordic Musculoskeletal Questionnaire (NMQ). The goal is to identify key risk factors and propose strategies for improving occupational health and safety.
METHODOLOGY
This study employed a quantitative, non-experimental approach characterized by a cross-sectional design and a descriptive–comparative scope. The non-experimental design enabled assessment of ergonomic conditions in the work environment without the manipulation of independent variables, while the cross-sectional perspective facilitated the analysis of workers’ postural exposure at a specific stage in the production process.
The comparative component of the study utilized the concurrent application of the RULA and ERIN methods to analyze similarities and potential differences in the classification of ergonomic risk associated with the evaluated work tasks. This methodological approach enhances the ability to compare the sensitivity of both methods concerning the characteristics of a production system marked by low levels of automation and a high degree of manual handling, conditions frequently observed in small-scale production units.
The researchers conducted the study in a water purification plant located in Mexico, characterized by predominantly manual operations and limited process automation. The production process comprises five primary operational stages: container internal cleaning, rinsing, filling, sealing (capping), and transport and storage. Tasks at these stations require manual handling of water containers weighing approximately 20 kg, as well as repetitive movements, trunk flexion, and sustained physical effort.
The analysis focuses on the postures adopted by operators during the execution of critical tasks within the work cycle, particularly those that impose heightened biomechanical demands.
Each workstation underwent a thorough analysis that considered the specific biomechanical challenges associated with task execution. At the internal cleaning and rinsing stations, operators engaged in repetitive upper limb movements characterized by shoulder flexion and extension, wrist deviation, and sustained trunk inclination. The filling station required moderate arm elevation, low force exertion, and minimal trunk involvement. At the labeling and sealing station, operators exhibited repetitive wrist flexion-extension and forearm pronation-supination. Finally, the transport station required manual handling of approximately 20 kg containers, involving trunk flexion, load lifting, and displacement while adopting asymmetric postures.
To assess the ergonomic conditions of the production process, this study utilized three complementary instruments: the Rapid Upper Limb Assessment (RULA) method, the Ergonomic Risk Index (ERIN), and the Nordic Musculoskeletal Questionnaire. Each tool facilitated the evaluation of different dimensions of ergonomic risk and musculoskeletal symptomatology among workers. The relationship between the instruments employed and the variables analyzed is presented in Table 1.
Extensive validation in the scientific literature supports the use of observational methods for ergonomic risk assessment. These approaches enable the evaluation of biomechanical exposure through systematic observations of workers’ postures, movement frequency, and the physical demands associated with various work tasks. According to Takala et al. (2010), these observational methods serve as practical and reliable tools for identifying risk factors for musculoskeletal disorders, especially in production environments characterized by low levels of automation, where direct instrumental measurement is often limited.
Building upon this methodological framework, the present study employs a combined application of the RULA and ERIN methods to assess postural load and evaluate the level of exposure to ergonomic risk throughout various stages of the production process. Furthermore, the analysis incorporates the Nordic Musculoskeletal Questionnaire to identify symptoms associated with musculoskeletal disorders.
Table 1
Instruments used for the assessment of ergonomic studies
|
Method |
Type of assessment |
Variables evaluated |
|
RULA |
Observational postural |
Postural assessment of the neck, trunk, upper |
|
ERIN |
Ergonomic risk index |
Movements of the trunk, arms, wrists, and neck; |
|
Nordic |
Epidemiological |
Presence of pain or discomfort in nine body regions |
Note. Based on “Standardised nordic questionnaires for the analysis of musculoskeletal symptoms,” by I. Kuorinka, B. Jonsson, A. Kilbom, H. Vintenberg, F. Biering-Sørensen, G. Andersson, and K. Jørgensen, 1987, Applied Ergonomics, 18(3), and “The Rapid Upper Limb Assessment (RULA): A survey method for the investigation of work-related upper limb disorders,” by L. McAtamney and E. N. Corlett, 1993, Applied Ergonomics, 18(3).
The Rapid Upper Limb Assessment (RULA) method evaluates the postural load affecting the upper limbs, neck, trunk, and legs during task performance. Developed by McAtamney and Corlett (1993), this method is an observational tool for identifying risk factors associated with work-related musculoskeletal disorders.
The application procedure consists of several stages: first, direct observation of activities at each workstation; second, photographic documentation of representative postures throughout the work cycle; third, identification of the most critical or unfavorable posture within each task; fourth, scoring based on the original RULA assessment tables; and finally, determination of the corresponding action level. Researchers categorized the final scores according to the method’s established levels, with the corresponding RULA action level classification presented in Table 2.
The application of RULA and ERIN involved a combination of direct observation and photographic recording. While photographs supported the documentation of representative postures; scoring primarily relied upon in-situ observation, facilitating the assessment of movement dynamics, work pace, and physical effort.
Table 2
RULA Method Rating Scale
|
Score |
Category |
Description |
|
1-2 |
Acceptable posture |
The evaluated posture does not pose a significant |
|
3-4 |
Requires revision |
The posture exhibits potential risk factors; therefore, |
|
5-6 |
Changes needed soon |
The posture reflects a moderate to high risk level; thus, |
|
7 |
Immediate intervention |
The posture poses a significant ergonomic risk; thus, |
Note. Adapted from “The Rapid Upper Limb Assessment (RULA): A survey method for the investigation of work-related upper limb disorders,” by L. McAtamney and E. N. Corlett, 1993, Applied Ergonomics, 18(3).
The Ergonomic Risk Index (ERIN) method serves as a complementary tool for assessing cumulative exposure to ergonomic risk associated with task execution. This method integrates seven key variables related to biomechanical exposure: trunk movement, arm movement, wrist movement, neck movement, work pace, level of physical effort, and worker self-perception.
Researchers evaluated each variable using the method’s predefined scale, which yields a cumulative score that facilitates the classification of ergonomic risk into four categories. The ERIN risk classification is detailed in Table 3.
Table 3
Classification of ergonomic risks according to the ERIN method
|
Score |
Risk level |
Explanation |
|
7-14 |
Low |
The postural and physical demands associated with the work |
|
15-23 |
Medium |
Ergonomic factors exist that may contribute to musculoskeletal |
|
24-35 |
High |
The work conditions involve substantial exposure to |
|
35 |
Very high |
There is a high likelihood of developing musculoskeletal |
Note. Adapted from “Systematic evaluation of observational methods assessing biomechanical exposures at work,” by E. P. Takala, I. Pehkonen, M. Forsman, G. Hansson, S. Mathiassen, W. Neumann, G. Sjøgaard, K. Veiersted, R. Westgaard, and J. Winkel, 2010, Scandinavian Journal of Work, Environment & Health, 36(1).
The inclusion of worker self-perception enhances objective biomechanical assessment, a factor recognized in ergonomic research as crucial for identifying occupational risks (Oakman et al., 2017).
To complement this analysis, researchers administered the Nordic Musculoskeletal Questionnaire (NMQ), a widely utilized tool in occupational health research for assessing the prevalence of musculoskeletal symptoms across various anatomical regions.
The Nordic Musculoskeletal Questionnaire was applied prior to implementing any ergonomic interventions to establish a baseline for identifying the prevalence of musculoskeletal symptoms associated with current working conditions.
The questionnaire facilitated the identification of pain, discomfort, or musculoskeletal symptoms in nine main anatomical regions. Table 4 presents the evaluated body regions.
Table 4
Assessment of anatomical regions utilizing the Nordic Musculoskeletal Questionnaire
|
Anatomical region |
Definition |
Description |
|
Neck |
Cervical region |
Evaluates discomfort associated with sustained |
|
Shoulders |
Scapulohumeral joints |
Identifies pain linked to repetitive arm elevation |
|
Elbows |
Elbow joints |
Assesses discomfort resulting from repetitive |
|
Wrists/Hands |
Distal upper limbs |
Identifies discomfort associated with gripping, |
|
Upper back |
Thoracic region |
Evaluates discomfort related to flexed or twisted |
|
Lower back |
Lumbar region |
Identifies pain associated with manual material |
|
Hips/Thighs |
Pelvic and femoral region |
Assesses the discomfort associated with |
|
Knees |
Knee joints |
Identifies the discomfort related to repetitive flexion |
|
Ankles/Feet |
Distal lower limbs |
Evaluates the discomfort associated with |
Note. Adapted from “Standardised nordic questionnaires for the analysis of musculoskeletal symptoms,” by I. Kuorinka, B. Jonsson, A. Kilbom, H. Vintenberg, F. Biering-Sørensen, G. Andersson, and K. Jørgensen, 1987, Applied Ergonomics, 18(3)
The evaluation of musculoskeletal symptoms occurred over two timeframes: the preceding 12 months and the last 7 days. This instrument has demonstrated high levels of reliability and validity in epidemiological studies aimed at identifying work-related musculoskeletal disorders (Crawford, 2007; Kuorinka et al., 1987).
The methodological procedure comprised four main stages:
1. Production process assessment: Researchers conducted initial observations at the selected workstations, identifying critical tasks and the periods of highest physical demand within the production cycle.
2. Observational recording: Researchers captured photographic documentation of worker postures during task execution at each workstation.
3. Application of ergonomic methods: Calculations for RULA and ERIN scores were performed independently for each workstation.
4. Comparative analysis: The risk levels obtained from both methods were compared to identify the similarities and differences in ergonomic risk classification.
To ensure consistency, the analysis focused on postures that correspond with instances of highest physical demand within the operational cycle.
The data analysis involved calculating individual scores for each workstation according to the different assessment methods. Researchers classified risk levels based on established criteria, and conducted qualitative comparisons of recommended action levels, and identified workstations with the greatest agreement in high or very high-risk classifications.
This approach facilitated the evaluation of each method’s ability to detect ergonomic risks in a small-scale, low-automation production system.
Participation in the study was voluntary for workers, and the confidentiality of the collected information was strictly upheld. The study was conducted solely for academic and ergonomic improvement purposes, ensuring that participants’ employment conditions or performance evaluations remained unaffected.
RESULTS
The implementation of the Ergonomic Risk Index (ERIN) facilitated the identification of the overall ergonomic risk associated with tasks performed at the five workstations within the production process. The findings demonstrated variability in risk exposure between work stations: those involving intensive manual handling of water containers and those requiring lower levels of physical demand. The scores for each workstation are presented in Table 5.
The results demonstrate that three out of the five evaluated workstations (1, 2, and 5) are categorized as high-risk, underscoring the necessity for immediate corrective measures. In contrast, the filling station exhibits the lowest risk level, while the labeling and sealing tasks are classified in a moderate risk range.
Table 5
Classification of ergonomic risks using the ERIN method
|
Station |
Activity |
ERIN Score |
Risk level |
|
1 |
Internal cleaning |
28 |
High |
|
2 |
Rinsing |
35 |
High |
|
3 |
Filling |
14 |
Low |
|
4 |
Labeling and sealing |
17 |
Medium |
|
5 |
Transport |
30 |
High |
A variable-specific analysis reveals that the primary contributors to the total score include arm posture and movement frequency, followed by physical effort and work pace, particularly observed while analyzing activities at the cleaning and transport stations.
The Rapid Upper Limb Assessment (RULA) method assessed the instantaneous postural load associated with tasks performed at each workstation, with particular emphasis on upper limb exposure. The results are presented in Table 6.
Table 6
Postural evaluation utilizing the RULA method
|
Station |
Activity |
RULA Score |
Risk level |
|
1 |
Interior cleaning |
6 |
High |
|
2 |
Rinse |
6 |
High |
|
3 |
Filling |
4 |
Medium |
|
4 |
Labeling and sealing |
4 |
Medium |
|
5 |
Transportation |
7 |
Very high |
The transport station manifested the highest risk level, necessitating immediate intervention. Likewise, the cleaning and rinsing stations require short-term ergonomic modifications. A segmented analysis identified the anatomical regions most impacted by postural load, specifically the wrist, forearm, and upper arm.
To identify consistencies and discrepancies in ergonomic risk classification, the researchers conducted a comparative analysis between the two methods. The results are presented in Table 7.
Table 7
A comparative analysis of the ERIN and RULA methods
|
Station |
ERIN Score |
ERIN Level |
RULA Score |
RULA Level |
Concordance |
|
1 |
28 |
High |
6 |
High |
Yes |
|
2 |
35 |
High |
6 |
High |
Yes |
|
3 |
14 |
Low |
4 |
Medium |
Partial |
|
4 |
17 |
Medium |
4 |
Medium |
Yes |
|
5 |
30 |
High |
7 |
Very High |
Yes (Critical) |
Alignment between both methods occurred in four out of the five workstations, while one workstation exhibited partial consistency. The primary discrepancy arose in the filling station, where ERIN classified the risk as low, whereas RULA indicated a moderate level of risk. This divergence can be attributed to methodological differences between the two tools; RULA emphasizes instantaneous postural assessment, whereas ERIN considers cumulative ergonomic risk exposure.
Building on the comparative findings from ERIN and RULA, researchers developed a graphical representation of the workstations evaluated to illustrate the postures, movements, and ergonomic risk levels identified at each stage of the production process. This representation is presented in Figure 1.
Figure 1
Comparative evaluation of ergonomic risk across workstations utilizing the ERIN and RULA methods.
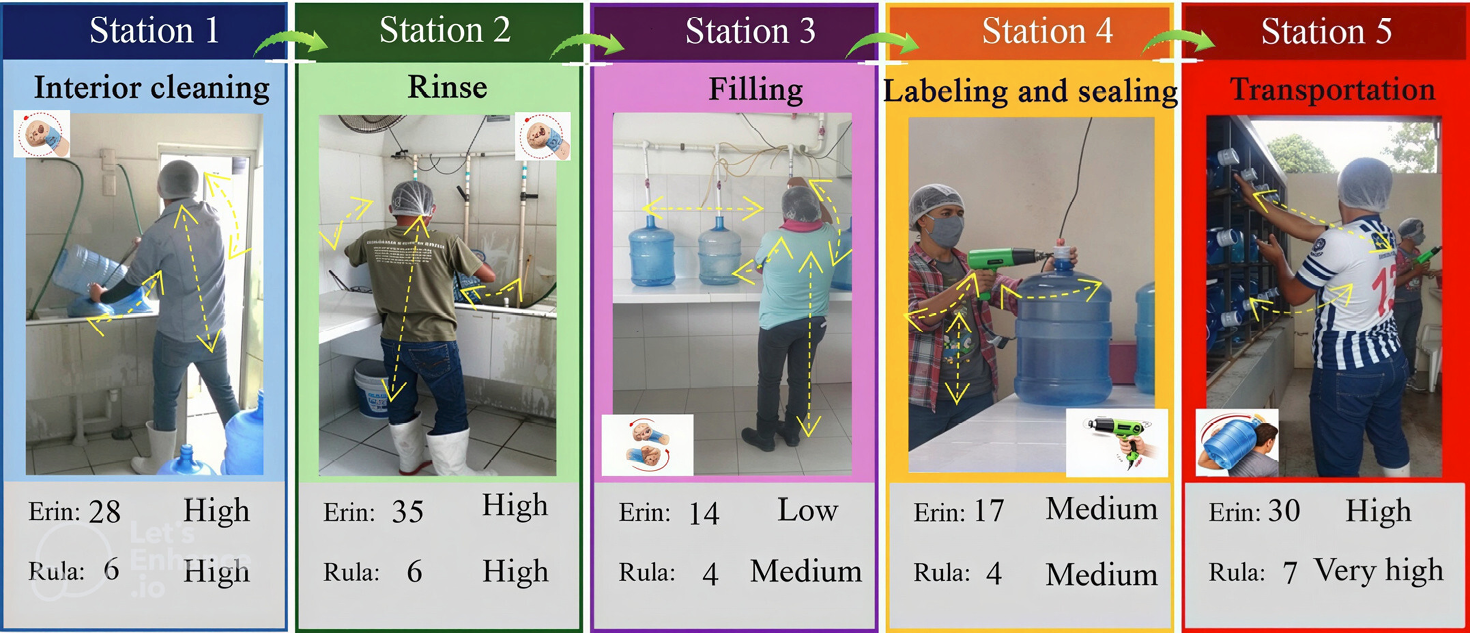
Note. The figure illustrates the five stages of the production process: internal cleaning, rinsing, filling, labeling and sealing, and transport/storage. The arrows highlight the primary postural movements observed during the execution of these tasks. The risk levels reflect the scores obtained from the ERIN and RULA applications.
The analysis identified the need for ergonomic interventions to reduce biomechanical risk exposure at the most critical workstations. Table 8 presents the projected improvements estimated using the ERIN method.
Table 8
Anticipated reduction in ergonomic risk by making operational improvements
|
Station |
Current Score |
Projected Score |
Change in risk level |
|
1 |
28 |
14 |
High → Low |
|
2 |
35 |
14 |
High → Low |
|
5 |
30 |
22 |
High → Medium |
Note. The authors provide an elaboration based on the expected outcomes if ergonomic interventions are implemented.
The proposed interventions include incorporating semi-automated bottle-washing systems to reduce repetitive manual scrubbing, implementing of conveyor- or roller-based transport systems to reduce manual load handling, and using mechanical lifting aids, such as lever systems or platforms, to facilitate container movement. Furthermore, it is essential to redesign workstations to optimize working height and reduce trunk flexion angles, thereby decreasing biomechanical strain on workers.
To identify the presence of musculoskeletal symptoms among workers, researchers administered the Nordic Musculoskeletal Questionnaire as a screening tool. The most frequently reported body regions included the wrist/hand, forearm, shoulder, and lower back.
The areas exhibiting the highest prevalence of symptoms corresponded to workstations classified as high or very-high-risk according to both the ERIN and RULA assessments, particularly in cleaning, rinsing, and transport tasks. At the transport station, multiple workers reported lower back discomfort due to the repetitive handling of approximately 20-kg containers. In contrast, the filling station, which ERIN classified as low risk, demonstrated a lower frequency of reported symptoms, indicating a consistency between observational ergonomic assessments and workers’ perceived discomfort.
Table 9 presents the prevalence of musculoskeletal symptoms identified through the Nordic Musculoskeletal Questionnaire.
Table 9
Assessment of the musculoskeletal symptoms reported using the Nordic Musculoskeletal Questionnaire
|
Body region |
Last 12 months (%) |
Last 7 days (%) |
|
Neck |
25 |
10 |
|
Shoulder |
40 |
20 |
|
Wrist/Hand |
60 |
35 |
|
Lower back |
55 |
30 |
Note. This study utilizes data collected through the application of the Nordic Musculoskeletal The questionnaire (NMQ) was administered to workers at the water purification plant. The methodology is adapted from “Standardised nordic questionnaires for the analysis of musculoskeletal symptoms,” by I. Kuorinka, B. Jonsson, A. Kilbom, H. Vintenberg, F. Biering-Sørensen, G. Andersson, and K. Jørgensen, 1987, Applied Ergonomics, 18(3).
DISCUSSION
The study’s findings reveal that workstations requiring intensive manual handling of loads present the highest levels of ergonomic risk. This observation aligns with prior research that links repetitive lifting and sustained trunk flexion to a higher incidence of lower back pain and musculoskeletal injuries in high-demand work environments (Da Costa & Ramos Vieira, 2010). In the evaluated process, the cleaning, rinsing, and transport stations require frequent handling of 20 kg water containers, thereby increasing exposure to biomechanical risk factors associated with musculoskeletal disorders (Graziosi et al., 2024).
The comparative application of RULA and ERIN demonstrates a strong consensus in identifying critical workstations, particularly stations 1, 2, and 5. This finding corroborates previous studies regarding the reliability of observational postural assessment tools. Kee (2022) noted that despite structural differences, these methods often converge in identifying tasks characterized by high physical workloads, particularly when upper-limb exposure is a factor. These results provide empirical evidence to support the combined use of observational ergonomic methods in production systems with limited automation.
Discrepancies emerged, particularly at the filling station, where ERIN classified the risk as low while RULA categorized it as moderate. This difference can be attributed to the distinct methodological approaches of each tool. RULA assesses the most demanding posture within the work cycle, while ERIN incorporates cumulative factors such as movement frequency, effort intensity, and work pace.
Numerous studies have indicated that observational methods often differ in their weighting of postural variables, applied force, and repetition, resulting in variations in risk classification for identical tasks (Grooten & Johansson, 2018; Yazdanirad et al., 2018). These findings underscore the importance of employing multiple assessment tools to achieve a more comprehensive evaluation of biomechanical exposure. Moreover, recent studies have emphasized the advantages of integrating multiple ergonomic approaches to improve the identification of musculoskeletal risk factors in tasks with a high physical workload (Jacquier-Bret & Gorce, 2024).
The Nordic Musculoskeletal Questionnaire facilitates a direct comparison between observational assessments and worker-reported symptoms. The anatomic regions exhibiting the highest prevalence of discomfort—namely the wrist, forearm, shoulder, and lower back--corresponded to workstations classified as high risk. This alignment underscores the validity of the ergonomic assessment and corresponds with studies that integrate postural and epidemiological approaches (Crawford, 2007; Koskas & Vignais, 2024).
From an intervention standpoint, recent evidence supports the anticipated reduction in risk following the implementation of operational improvements and mechanical aids. Rivilis et al. (2008) demonstrated that ergonomic interventions can significantly reduce musculoskeletal disorders when modifications are applied to work design. Similarly, recent systematic reviews indicate that interventions aimed at task redesign and work organization can effectively reduce the prevalence of these disorders (Santos et al., 2025).
Overall, these findings confirm that the combined application of RULA, ERIN, and the Nordic Musculoskeletal Questionnaire enables a more precise identification of critical ergonomic risk factors in labor-intensive processes. This methodological triangulation enhances decision-making regarding workstation redesign and plays a key role in the prevention of musculoskeletal disorders. Workstation redesign also helps to improve working conditions in environments characterized by low automation.
This study addresses the gap between observational and epidemiological ergonomic assessments in small-scale production systems, a domain that remains underrepresented in the current scientific literature.
CONCLUSIONS
The comparative assessment using the RULA and ERIN methods revealed distinct differences in ergonomic risk levels across the five workstations involved in the artisanal water bottling process. The cleaning, rinsing, and transport stations exhibited the highest exposure levels, classified as high or very high risk, which confirms the presence of biomechanical conditions that may contribute to the development of musculoskeletal disorders among workers.
The agreement between the two methods enhances the validity of the ergonomic diagnosis. However, the disparities identified at the filling station underscore the unique sensitivities of the RULA and ERIN methods. While RULA tends to react more critically to extreme postures at specific moments in the work cycle, ERIN incorporates cumulative variables related to work pace and perceived exertion. This methodological complementarity facilitates a more comprehensive analysis of ergonomic risk exposure.
Furthermore, the integration of the Nordic Musculoskeletal Questionnaire corroborated the correlation between observed postural exposure and the musculoskeletal symptoms reported by workers, reinforcing the consistency of the findings obtained through ergonomic evaluation methods.
The projected improvements suggest that relatively low-cost operational interventions--such as the introduction of mechanical aids for container transport, adjustments in workstation design, and the partial automation of specific operations--can significantly reduce overall ergonomic risk levels in the most critical workstations.
Ultimately, the combined use of RULA, ERIN, and the Nordic Musculoskeletal Questionnaire constitutes a viable and replicable methodology for ergonomic assessment in micro and small enterprises characterized by labor-intensive processes. In this context, ergonomics should be regarded not only as a strategy for preventing occupational risks but also as a tool for enhancing operational efficiency and promoting the sustainability of production systems. This study contributes empirical evidence from a sector that remains underrepresented in the scientific literature: small-scale water purification plants operating with manual production processes. The findings may serve as a foundation for future longitudinal research to evaluate the long-term impact of ergonomic interventions in similar production environments.
From a methodological standpoint, the Rapid Upper Limb Assessment (RULA) exhibited heightened sensitivity to instantaneous postural overload, particularly in tasks that require extreme upper-limb positions. In contrast, the Ergonomic Risk Identification Network (ERIN) provides a more comprehensive evaluation by incorporating cumulative factors, including work pace, effort intensity, and worker perception. While RULA is advantageous for rapid postural screening, ERIN facilitates a more extensive assessment of overall ergonomic exposure. Therefore, the combined application of both methods is recommended to achieve a more complete ergonomic diagnosis.
Despite the contributions of this research, several methodological limitations should be recognized. First, the cross-sectional design limited the ability to evaluate ergonomic conditions over time, constraining the capacity to establish causal relationships between exposure to risk factors and the development of musculoskeletal disorders.
Second, conducting the study in a single water purification plant with specific production characteristics may restrict the generalizability of the results. The same results may not apply to other industrial contexts with different levels of automation or operational configurations.
Furthermore, while the combination of RULA, ERIN, and the Nordic Musculoskeletal Questionnaire offers a comprehensive assessment of ergonomic risk, observational methods can introduce variability in posture interpretation. Nevertheless, employing multiple complementary instruments enhances the consistency of the ergonomic diagnosis.
Finally, the Nordic Questionnaire depends on workers to report their own musculoskeletal symptoms. These reports can be affected by personal factors and how individuals perceive pain. However, when combined with methods that assess posture, these self-reports provide a way to compare epidemiological data with the actual biomechanical exposure that occurs in the workplace.
Future research could broaden the analysis through longitudinal studies that evaluate the progression of musculoskeletal disorders over time and assess the effectiveness of specific ergonomic interventions in production systems characterized by intensive manual material handling.
The results of this study hold significant implications for ergonomic management in micro and small enterprises characterized by labor-intensive processes. The identification of critical workstations through the combined application of the RULA and ERIN methods enabled the establishment of intervention priorities to reduce exposure to biomechanical risk factors.
In this light, ergonomics can serve as a strategic tool not only for preventing musculoskeletal disorders but also for enhancing productivity and promoting operational sustainability in production systems with low levels of automation.
CONFLICTS OF INTEREST
The authors affirm they have no conflicts of interest related to the conduct or publication of this study.
AUTHOR CONTRIBUTION
Reina Verónica Román Salinas: conceptualization, formal analysis, research, methodology, project administration, resources, validation, visualization, writing–original draft, writing–review and editing. Marco Antonio Díaz Martínez: conceptualization, formal analysis, research, project administration, resources, supervision, validation, visualization, writing–original draft, writing–review and editing. Víctor Hugo Tobías Martínez: research, methodology, project administration, supervision, visualization, writing–original draft, writing–review and editing. Edgar Jearvavi Vázquez Moreno: formal analysis, methodology, resources, supervision, validation, visualization, writing–original draft, writing–review and editing. Rubén Jérez Calderón: research, resources, validation, visualization, writin–original draft, writing–review and editing.
DECLARATION ON THE USE OF GENERATIVE IA
The authors used generative AI tools solely to improve the writing, grammar, and clarity of the manuscript. The interpretation of the results, analysis, and conclusions correspond exclusively to the authors.
REFERENCES
Ansari, N. A., & Sheikh, M. J. (2014). Evaluation of work posture by RULA and REBA: A case study. IOSR Journal of Mechanical and Civil Engineering, 11(4), 18-23. https://doi.org/10.9790/1684-11431823
Baklouti, S., Chaker, A., Rezgui, T., Sahbani, A., Bennour, S., & Laribi, M. A. (2024). A novel IMU-based system for work-related musculoskeletal disorders risk assessment. Sensors, 24(11), Article 3419. https://doi.org/10.3390/s24113419
Conforti, I., Mileti, I., Del Prete, Z., & Palermo, E. (2019, 4-6 June). Assessing ergonomics and biomechanical risk in manual handling of loads through a wearable system [Paper presentation]. 2019 II Workshop on Metrology for Industry 4.0 and IoT (MetroInd4.0&IoT), Naples, Italy. https://doi.org/10.1109/METROI4.2019.8792843
Crawford, J. O. (2007). The nordic musculoskeletal questionnaire. Occupational Medicine, 57(4), 300-301. https://doi.org/10.1093/occmed/kqm036
Da Costa, B. R., & Ramos Vieira, E. (2010). Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies. American Journal of Industrial Medicine, 53(3), 285-323. https://doi.org/10.1002/ajim.20750
Demissie, B., Bayih, E. T., & Demmelash, A. A. (2024). A systematic review of work-related musculoskeletal disorders and risk factors among computer users. Heliyon, 10(3), Article e25075. https://doi.org/10.1016/j.heliyon.2024.e25075
Graziosi, F., Bonfiglioli, R., Decataldo, F., & Violante, F. S. (2024). Criteria for assessing exposure to biomechanical risk factors: A research-to-practice guide-part 1: General issues and manual material handling. Life, 14(11), Article 1398. https://doi.org/10.3390/life14111398
Grooten, W. J. A., & Johansson, E. (2018). Observational methods for assessing ergonomic risks for work-related musculoskeletal disorders: A scoping review. Revista Ciencias de la Salud, 16(special), 8-38. https://doi.org/10.12804/revistas.urosario.edu.co/revsalud/a.6840
Jacquier-Bret, J., & Gorce, P. (2024). Work-related musculoskeletal disorders risk assessment during manual lymphatic drainage with compression bands among physiotherapists. Healthcare, 12(1), Article 118. https://doi.org/10.3390/healthcare12010118
Kee, D. (2022). Systematic comparison of OWAS, RULA and REBA based on a literature review. International Journal of Environmental Research and Public Health, 19(1), Article 595. https://doi.org/10.3390/ijerph19010595
Koskas, D., & Vignais, N. (2024). Physical ergonomic assessment in cleaning hospital perating rooms based on inertial measurement units. Bioengineering, 11(2), Article 54. https://doi.org/10.3390/bioengineering11020154
Kuorinka, I., Jonsson, B., Kilbom, Å., Vinterberg, H., Biering-Sørensen, F., Andersson, G., & Jørgensen, K. (1987). Standardised nordic questionnaires for the analysis of musculoskeletal symptoms. Applied Ergonomics, 18(3), 233-237. https://doi.org/10.1016/0003-6870(87)90010-X
McAtamney, L., & Corlett, E. N. (1993). RULA: A survey method for the investigation of work-related upper limb disorders. Applied Ergonomics, 24(2), 91-99. https://doi.org/10.1016/0003-6870(93)90080-S
Muhacir, D., Aktaş, M. i., & Özceylan, E. (2022). REBA and RULA ergonomic risk assessments of operators in a maintenance and repair workshop of a textile factory. Acta Technica Napocensis, 65(3S), 759-768. https://atna-mam.utcluj.ro/index.php/Acta/article/view/1960/1559
Oakman, J., Neupane, S., Proper, K., Kinsman, N., & Nygård, C-H. (2017). Workplace interventions to improve work ability: A systematic review and meta-analysis of their effectiveness. Scandinavian Journal of Work, Environment & Health, 44(2), 134-146. https://doi.org/10.5271/sjweh.3685
Rivilis, I., Van Eerd, D., Cullen, K., Cole, D. C., Irvin, E., Tyson, J., & Mahood, Q. (2008). Effectiveness of participatory ergonomic interventions on health outcomes: A systematic review. Applied Ergonomics, 39(3), 342-358. https://doi.org/10.1016/j.apergo.2007.08.006
Santos, W., Rojas, C., Isidoro, R., Lorente, A., Dias, A., Mariscal, G., Benlloch, M., & Lorente, R. (2025). Efficacy of ergonomic interventions on work-related musculoskeletal pain: A systematic review and meta-analysis. Journal of Clinical Medicine, 14(9), Article 3034. https://doi.org/10.3390/jcm14093034
Soares, D., Bernardes, L., & Nicodemo, D. (2026). Ergonomics in manual lifting and load handling: A literature review on biomechanical risks and technologies for the prevention of musculoskeletal disorders. Research, Society and Development, 15(1), Article e6615150485. https://doi.org/10.33448/rsd-v15i1.50485
Takala, E. P., Pehkonen, I., Forsman, M., Hansson, G. Å., Mathiassen, S. E., Neumann, W. P., Sjøgaard, G., Veiersted, K. B., Westgaard, R. H., & Winkel, J. (2010). Systematic evaluation of observational methods assessing biomechanical exposures at work. Scandinavian Journal of Work, Environment & Health, 36(1), 3-24. https://doi.org/10.5271/sjweh.2876
Yang, F., Di, N., Guo, W-w., Ding, W-b., Jia, N., Zhang, D., Li, D., Wang, D., Wang, R., Zhang, Liu, Y., Shen, B., Wang, Z-x., & Yin, Y. (2023). The prevalence and risk factors of work-related musculoskeletal disorders among electronics manufacturing workers: A cross-sectional analytical study in China. BMC Public Health, 23(10), Article 10. https://doi.org/10.1186/s12889-022-14952-6
Yazdanirad, S., Khoshakhlagh, A. H., Habibi, E., Zare, A., Zeinodini, M., & Dehghani, F. (2018). Comparing the effectiveness of three ergonomic risk assessment methods ―RULA, LUBA, and NERPA― to predict the upper extremity musculoskeletal disorders. Indian Journal of Occupational and Environmental Medicine, 22(1), 17-21. https://journals.lww.com/ijoe/fulltext/2018/22010/comparing_the_effectiveness_of_three_ergonomic.5.aspx